[vc_row][vc_column][vc_single_image image=”491531″ img_size=”full” alignment=”center”][/vc_column][/vc_row][vc_row][vc_column][mk_padding_divider][/vc_column][/vc_row][vc_row][vc_column][vc_column_text css=”.vc_custom_1679506139819{margin-bottom: 0px !important;}”]A menstrual period is the monthly shedding of the uterine lining. Menstruation is also known by the terms menses, menstrual period, menstrual cycle or period. Menstruation is a normal and healthy part of life for most people with a uterus and no matter what you think you know about it age, hormones or even the weather can change how a person menstruates and how it feels ( A reason for why connecting with a Fertility Doula is a good idea!). Period facts are often obscured by myths about menstruation. Most people with a uterus get their first period between the ages of 10 and 15 and continue to have their period until their late 40s or early 50s.
So let’s talk about some period facts:
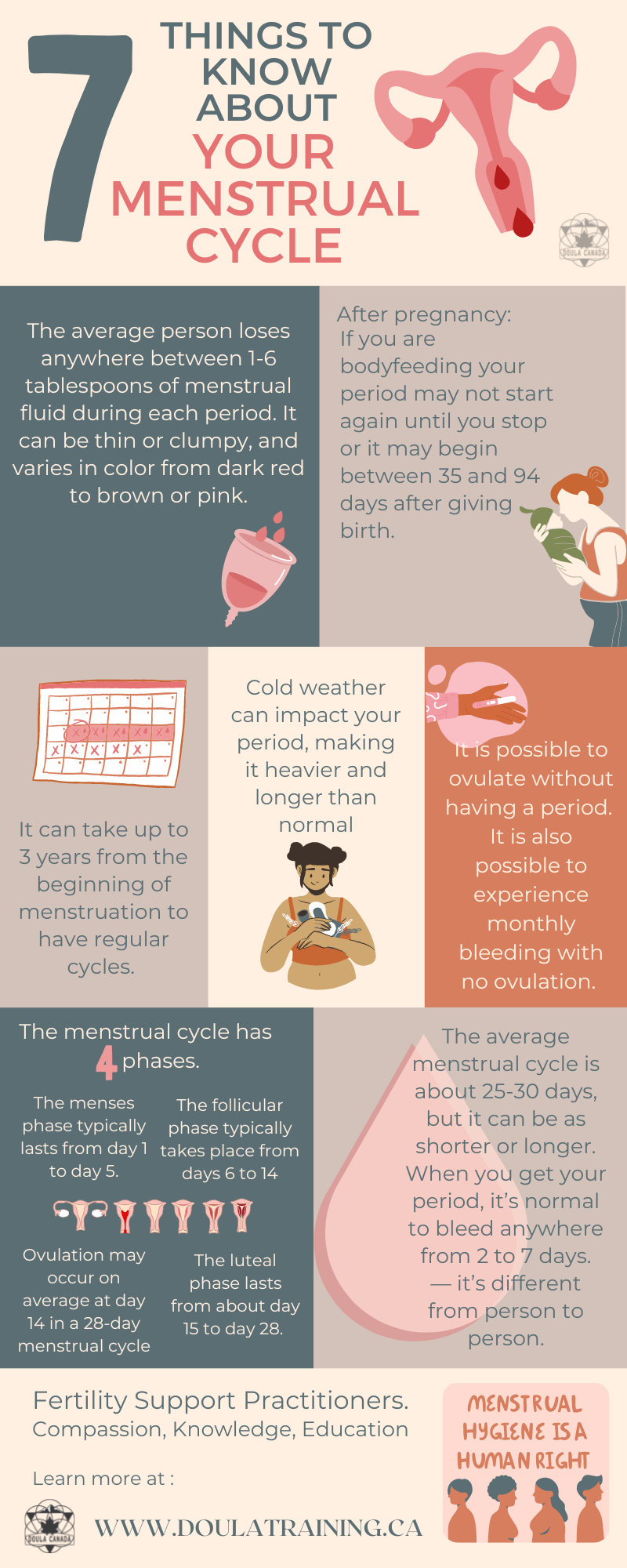
- You loose less blood than you think you do: First off, you need to know that only approx. 50% of menstrual fluid is blood. ‘Menstrual fluid’ is not the same as ‘blood’, menstrual fluid also contains cervical mucous and vaginal secretions. On average a person loses anywhere between 1-6 tablespoons of menstrual fluid during each period. It can be thin or clumpy and varies in colour from dark red to brown or pink.
- It can take up to 3 years from the beginning of menstruation for your period to become regular: It’s common for cycles to be somewhat unpredictable for about two years after the first period. This means periods may not always come at the same time every cycle. Your periods may also look and feel somewhat different cycle-to-cycle. The first period may be quite short, with only a little bit of bleeding and the second period may be longer with more bleeding. After a couple of years, your cycles should become more regular, but may still continue to vary. Most cycles settle into a predictable rhythm about six years after menarche (the onset of your period).
- The average menstrual cycle is about 25- 30 days but not always: The average length of a menstrual cycle is 28 days. The days between periods is your menstrual cycle length. However, a cycle can range in length from 21 days to about 35 days and still be normal. Most people have their period (bleed) for between three and seven days. Once you reach your 20s, your cycles become more consistent and regular. Once your body begins transitioning to menopause, your periods will change again and become more irregular. From the time of your first cycle to menopause, the average menstruating person will have around 450 periods in their lifetime. Added up, this equates to around 10 years — or about 3,500 days — of the average menstruating person ’s life that will be spent menstruating.
- Steps of your Cycle: The rise and fall of your hormones trigger the steps in your menstrual cycle. Your hormones cause the organs of your reproductive tract to respond in certain ways. The specific events that occur during your menstrual cycle are:
- The menses phase: This phase, which typically lasts from day one to day five, is the time when the lining of your uterus sheds through your vagina if pregnancy hasn’t occurred. Most people bleed for three to five days, but a period lasting only three days to as many as seven days is usually not a cause for worry.
- The follicular phase: This phase typically takes place from days six to 14. During this time, the level of the hormone estrogen rises, which causes the lining of your uterus (the endometrium) to grow and thicken. In addition, another hormone — follicle-stimulating hormone (FSH) — causes follicles in your ovaries to grow. During days 10 to 14, one of the developing follicles will form a fully mature egg (ovum).
- Ovulation: This phase occurs roughly at about day 14 in a 28-day menstrual cycle. A sudden increase in another hormone — luteinizing hormone (LH) — causes your ovary to release its egg. This event is ovulation. However, some people do not ovulate or they ovulate at different times, more about this later.
- The luteal phase: This phase lasts from about day 15 to day 28. Your egg leaves your ovary and begins to travel through your fallopian tubes to your uterus. The level of the hormone progesterone rises to help prepare your uterine lining for pregnancy. If the egg becomes fertilized by sperm and attaches itself to your uterine wall (implantation), you become pregnant. If pregnancy doesn’t occur, estrogen and progesterone levels drop and the thick lining of your uterus sheds during your period.
- Let’s talk about ovulation: Ovulation usually happens once each month, about two weeks before your next period. Ovulation can last from 16 to 32 hours. It is possible to get pregnant in the five days before ovulation and on the day of ovulation, but it’s more likely in the three days leading up to and including ovulation. Once the egg is released, it will survive up to 24 hours. If sperm reaches the egg during this time, you may get pregnant. Some people with a uterus do not ovulate regularly. This is common in the first two to three years after your periods start and during the lead-up to menopause. Some conditions, such as polycystic ovary syndrome (PCOS) and amenorrhoea (when periods stop due to excessive exercise or eating disorders) may cause irregular ovulation. Individuals with certain hormone conditions do not ovulate at all. It is possible to ovulate and not have a period after. It is possible to get pregnant without having periods in several months, but the chance of pregnancy of much lower when you are not having periods, compared to when you have regular periods. It is also possible to experience monthly periods without going through ovulation first- this is considered abnormal and is the result of something called an “anovulatory cycle”.
- Your periods get worse when it is cold: This is definitely an amazing period fact: cold weather can impact your period, making it heavier and longer than normal. During the winter months, a menstruating person’s flow, period duration, and even pain level are longer than in the summer. This pattern also extends to women who live in colder climates rather than warmer temperatures. The seasons can also affect your PMT too — the darker, shorter days can adversely impact your mood when combined with female productive hormones. This is thought to be because of a lack of sunshine, which helps our bodies to produce vitamin D and dopamine — which both boost our moods, happiness, concentration and all-around health levels.
- Periods after Pregnancy: After birth, your periods will return at your body’s own pace. It’s possible for your periods to return as soon as 4 to 6 weeks after childbirth. If you bottle feed or partially bodyfeed your baby, you’ll tend to start having periods sooner than if you exclusively bodyfeed. If you choose to bodyfeed exclusively, your first period may not return for several months. For those who keep bodyfeeding, it might not return for 1 to 2 years. The range of “normal”, is enormous. Experiencing a menstrual period does not mean that your menstrual cycle has returned permanently and without an accurate clinical test, you won’t know whether or not you ovulated (released an egg and could potentially become pregnant). You are more likely to ovulate and resume regular periods if your baby is going for more than a few hours without breastfeeding (for instance, at night) and your baby is more than 6 months old. Many bodyfeeding parents experience a time of delayed fertility during breastfeeding. This is very common and is referred to in many places as the Lactation Amenorrhea Method (LAM) of contraception. However it is important to remember that you can get pregnant while nursing, even without a period.
These 7 facts are just the tip of the iceburg when it comes to understanding your body and menstruation. If you have questions, whether you are trying to get pregnant or not a Fertility Doula can help with that![/vc_column_text][/vc_column][/vc_row][vc_row][vc_column][mk_padding_divider][/vc_column][/vc_row][vc_row][vc_column][vc_single_image image=”491536″ img_size=”medium”][/vc_column][/vc_row][vc_row][vc_column][vc_btn title=”Download the infographic here” color=”turquoise” link=”url:https%3A%2F%2Fstefanie-techops.wisdmlabs.net%2Fwp-content%2Fuploads%2F2023%2F03%2F7-things-to-know-about-your-cycle-1.pdf|target:_blank”][/vc_column][/vc_row]




 Meet Sarah Alicia Elder. Owner of ElderFlower Doula Serving families in New Westminster B.C Canada, This mother of three, can’t stay still and her love for learning has opened up many different career paths. Her sense of community has led her to different fields within human services. Now, Sarah is putting it all together to help families in New Westminster. She is a full-service doula-in-training offering support and resources for pre-pregnancy to post-partum and everything in-between.
Meet Sarah Alicia Elder. Owner of ElderFlower Doula Serving families in New Westminster B.C Canada, This mother of three, can’t stay still and her love for learning has opened up many different career paths. Her sense of community has led her to different fields within human services. Now, Sarah is putting it all together to help families in New Westminster. She is a full-service doula-in-training offering support and resources for pre-pregnancy to post-partum and everything in-between.
 You can learn more about Sarah Alicia here
You can learn more about Sarah Alicia here